
Vaginitis is infectious or noninfectious inflammation of the vaginal mucosa, sometimes with inflammation of the vulva. Symptoms include vaginal discharge, irritation, pruritus, and erythema. Diagnosis is by testing of vaginal secretions. Treatment is directed at the cause and at any severe symptoms.
The most common causes of vaginitis vary by patient age. Vulvitis and vulvovaginitis have some of the same causes.
In children, vaginitis usually involves infection with gastrointestinal tract flora (nonspecific vulvovaginitis). A common contributing factor in girls aged 2 to 6 years is poor perineal hygiene (eg, wiping from back to front after bowel movements; not washing hands after bowel movements; fingering, particularly in response to pruritus).
Chemicals in bubble baths or soaps may cause inflammation.
Foreign bodies (eg, tissue paper) may cause nonspecific vaginitis with a bloody discharge.
Sometimes childhood vulvovaginitis is due to infection with a specific pathogen (eg, streptococci, staphylococci, Candida species; occasionally, pinworm).
Sexual abuse can result in sexually transmitted diseases, including trichomonal vaginitis, in children.
In women of reproductive age, vaginitis is usually infectious. The most common types are
Normally in women of reproductive age, Lactobacillus sp is the predominant constituent of normal vaginal flora. Colonization by these bacteria keeps vaginal pH in the normal range (3.8 to 4.2), thereby preventing overgrowth of pathogenic bacteria. Also, high estrogen levels maintain vaginal thickness, bolstering local defenses.
Factors that predispose to overgrowth of bacterial vaginal pathogens may include the following:
Vaginitis may result from foreign bodies (eg, forgotten tampons). Inflammatory vaginitis, which is noninfectious, is uncommon.
In postmenopausal women, a marked decrease in estrogen usually causes vaginal thinning, increasing vulnerability to infection and inflammation. Some treatments (eg, oophorectomy, pelvic radiation, certain chemotherapy drugs) also result in loss of estrogen. Decreased estrogen predisposes to inflammatory (particularly atrophic) vaginitis.
Hormonal changes during menopause can result in a more alkaline vaginal pH, which can predispose to overgrowth of vaginal pathogenic bacteria.
Poor hygiene (eg, in patients who are incontinent or bedbound) can lead to chronic vulvar inflammation due to chemical irritation from urine or feces or due to nonspecific infection.
Bacterial vaginosis, candidal vaginitis, and trichomonal vaginitis are uncommon among postmenopausal women but may occur in those with risk factors.
At any age, conditions that predispose to vaginal or vulvar infection include
Noninfectious vulvitis accounts for up to 30% of vulvovaginitis cases. It may result from hypersensitivity or irritant reactions to hygiene sprays or perfumes, menstrual pads, laundry soaps, bleaches, fabric softeners, fabric dyes, synthetic fibers, bathwater additives, toilet tissue, or, occasionally, spermicides, vaginal lubricants or creams, latex condoms, vaginal contraceptive rings, or diaphragms.
Vaginitis causes vaginal discharge, which must be distinguished from normal discharge. In children, normal discharge is common when estrogen levels are high—eg, during the first 2 weeks of life because maternal estrogen is transferred before birth (slight bleeding often occurs when estrogen levels abruptly decrease) and during the few months before menarche, when estrogen production increases.
Normal vaginal discharge is commonly milky white or mucoid, odorless, and nonirritating; it can result in vaginal wetness that dampens underwear.
Discharge due to vaginitis is accompanied by pruritus, erythema, and sometimes burning, pain, or mild bleeding. Pruritus may interfere with sleep. Dysuria or dyspareunia may occur. In atrophic vaginitis, discharge is scant, dyspareunia is common, and vaginal tissue appears thin and dry. Although symptoms vary among particular types of vaginitis, there is much overlap (see table Common Types of Vaginitis).TABLECommon Types of Vaginitis
Speculum Examination in Vaginitis
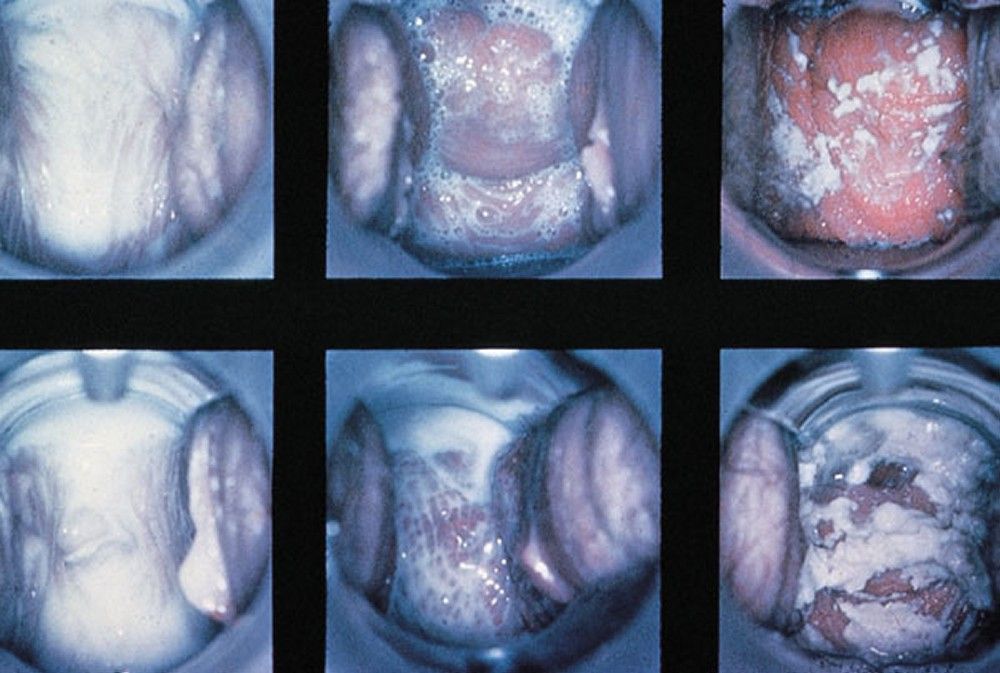
BY PERMISSION OF THE PUBLISHER. FROM SPITZER M, MANN M. IN ATLAS OF CLINICAL GYNECOLOGY: GYNECOLOGIC PATHOLOGY. EDITED BY M STENCHEVER (SERIES EDITOR) AND B GOFF. PHILADELPHIA, CURRENT MEDICINE, 1998. (COURTESY OF THE INTERNATIONAL SOCIETY FOR THE STUDY OF VULVAR DISEASE, FROM THE COLLECTION OF THE LATE DR. HERMAN GARDNER.)
Vulvitis can cause erythema, pruritus, and sometimes tenderness and discharge from the vulva.
Vaginitis is diagnosed using clinical criteria and in-office or laboratory testing.
First, vaginal secretions are obtained with a water-lubricated speculum, and pH paper is used to measure pH in 0.2 intervals from 4.0 to 6.0. Then, secretions are placed on 2 slides with a cotton swab and diluted with 0.9% sodium chloride on one slide (saline wet mount) and with 10% potassium hydroxide on the other (KOH wet mount). The KOH wet mount is checked for a fishy odor (whiff test), which results from amines produced in trichomonal vaginitis or bacterial vaginosis. The saline wet mount is examined microscopically as soon as possible to detect trichomonads, which can become immotile and more difficult to recognize within minutes after slide preparation. Potassium hydroxide dissolves most cellular material except for yeast hyphae, making identification easier.
Clinical criteria and in-office testing are the most cost-effective way to diagnose infectious vaginitis. However, if findings are inconclusive, the discharge may be cultured for fungi or trichomonads. Also, some relatively new diagnostic tests are commercially available for clinical use (1–5).
Other causes of discharge are ruled out:
Vaginal Secretions for Wet Mount Specimen

BY PERMISSION OF THE PUBLISHER. FROM JUDSON F. IN ATLAS OF INFECTIOUS DISEASES: SEXUALLY TRANSMITTED DISEASES. EDITED BY G MANDELL (SERIES EDITOR) AND MF REIN. PHILADELPHIA, CURRENT MEDICINE, 1996.Wet Mount (Normal)

BY PERMISSION OF THE PUBLISHER. FROM HILLIER S. IN ATLAS OF INFECTIOUS DISEASES: SEXUALLY TRANSMITTED DISEASES. EDITED BY G MANDELL (SERIES EDITOR) AND MF REIN. PHILADELPHIA, CURRENT MEDICINE, 1996.Trichomonads on Wet Mount

IMAGE OBTAINED FROM THE PUBLIC HEALTH IMAGE LIBRARY OF THE CENTERS FOR DISEASE CONTROL AND PREVENTION.
If children have trichomonal vaginitis, evaluation for sexual abuse is required. If they have unexplained vaginal discharge, cervicitis, which may be due to a sexually transmitted disease, should be considered. If women have bacterial vaginosis or trichomonal vaginitis (and thus are at increased risk of sexually transmitted diseases), cervical tests for Neisseria gonorrhoeae and Chlamydia trachomatis, common causes of sexually transmitted PID, are done.
The vulva should be kept as clean as possible. Soaps and unnecessary topical preparations (eg, feminine hygiene sprays) should be avoided. Intermittent use of ice packs or warm sitz baths with or without baking soda may reduce soreness and pruritus.
If symptoms are moderate or severe or do not respond to other measures, drugs may be needed. For pruritus due to noninfectious conditions, topical corticosteroids (eg, topical 1% hydrocortisone twice a day as needed) can be applied to the vulva but not in the vagina. Oral antihistamines decrease pruritus and cause drowsiness, helping patients sleep.
Any infection (eg, bacterial vaginosis, candidal vaginitis, trichomoniasis) or other cause is treated. Foreign bodies are removed.
Prepubertal girls are taught good perineal hygiene (eg, wiping front to back after bowel movements and voiding, washing hands, avoiding fingering the perineum). If chronic vulvar inflammation is due to being bedbound or incontinent, better vulvar hygiene may help.









